Drug restores hair growth in patients with alopecia areata
EXCERPT FROM COLUMBIA UNIVERSITY MEDICAL CENTER
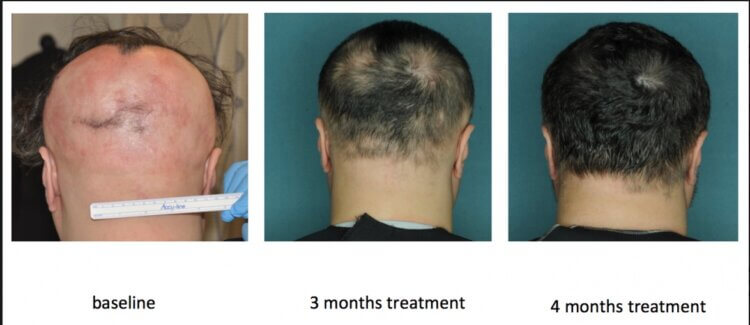
photo credit: Columbia University Medical Center / Hair Regrowth After Ruxolitinib in Alopecia Areata
Seventy-five percent of patients with moderate to severe alopecia areata—an autoimmune disease that causes patchy, and less frequently, total hair loss—had significant hair regrowth after treatment with ruxolitinib, reported researchers from Columbia University Medical Center (CUMC). By the end of their treatment, average hair regrowth was 92 percent.
Findings from an open-label clinical trial of 12 patients with alopecia areata were published today in the Journal of Clinical Investigation/Insight, alongside a paper reporting results of a separate study from Stanford University and Yale University that tested a similar drug.
“Although our study was small, it provides crucial evidence that JAK inhibitors may constitute the first effective treatment for people with alopecia areata,” said Julian Mackay-Wiggan, MD, MS, associate professor and director of the clinical research unit in dermatology at CUMC and a dermatologist at NewYork-Presbyterian/Columbia. “This is encouraging news for patients who are coping with the physical and emotional effects of this disfiguring autoimmune disease.”
Alopecia areata, the second most common form of hair loss, can occur at any age and affects men and women equally. The disease usually causes hair loss on the scalp, but some patients also experience facial and body hair loss, with devastating consequences particularly in children. Currently, there are no known treatments that can completely restore hair. Previously, the Columbia researchers identified the specific immune cells and the dominant inflammatory signaling pathways responsible for attacking the hair follicle in alopecia areata, putting them into a dormant state. Subsequent experiments with mouse and human hair follicles showed that topical and oral drugs that inhibit the Janus kinase (JAK) family of enzymes, known as JAK inhibitors, reawaken these dormant follicles by blocking inflammatory signaling. Two such JAK inhibitors already approved by the U.S. FDA are ruxolitinib, a medication that is used to treat bone marrow malignancies, and tofacitinib, a treatment for rheumatoid arthritis.
“These disorders are both characterized by dysregulated signaling pathways, similar to alopecia areata, which is dominated by the interferon signaling pathway. Even though the diseases are very different, this common feature gave us the initial idea to test JAK inhibitors in people with alopecia,” said Raphael Clynes, MD, PhD, adjunct associate professor of dermatology at CUMC.
To test this hypothesis, the researchers initiated a small, open-label clinical trial of 12 patients with moderate to severe alopecia areata (more than 30 percent hair loss). All patients were given 20 mg of oral ruxolitinib, twice a day, for 3 to 6 months. Participants were followed for an additional 3 months to assess the durability of treatment response.
Nine of the patients had hair regrowth of 50 percent or greater. By the end of the treatment period, 77 percent of those who responded to the therapy achieved hair regrowth of over 95 percent. A third of the responders had significant hair loss in the follow-up period after the medication was stopped, although their hair loss did not reach pre-treatment levels.
Skin biopsies performed before, during, and after treatment also revealed that responders had a reduction in levels of interferon signaling and cytotoxic T lymphocytes—indicators of an inflammatory response—and higher levels of hair keratins, which are proteins that indicate hair growth. These levels were similar to those in people without alopecia areata. Before starting treatment, patients who ultimately did not respond to therapy had lower levels of inflammatory signatures, suggesting that it may be possible to distinguish between responders and nonresponders.
“We are very excited about the use of biomarkers to follow the response of patients to this treatment,” said Angela M. Christiano, PhD, the Richard and Mildred Rhodebeck Professor of Dermatology and professor of genetics and development at CUMC. “This will allow us to so monitor improvements in their gene expression signatures even before hair growth appears.”
The drug was well-tolerated in all participants, with no serious adverse events. Those that did occur were infrequent, and included bacterial skin infections, skin allergy symptoms, and lower hemoglobin levels, which resolved with dose adjustment.”Our findings suggest that initial treatment induces a high rate of disease remissions in patients with moderate to severe alopecia areata but maintenance therapy may be needed,” said Dr. Mackay-Wiggan. “While larger, randomized trials are needed to confirm the safety and efficacy of ruxolitinib in people with moderate to severe alopecia areata, our initial results are very encouraging.”
In the Stanford/Yale study, a series of patients with moderate to severe alopecia areata responded to another JAK inhibitor called tofacitinib. “Together, the two studies show that we’re on the right track,” said Dr. Christiano, who is a co-author of the tofacitinib paper.
The CUMC research team plans to expand their studies to include testing these drugs in other conditions such as vitiligo, scarring alopecias and androgenetic alopecia (pattern baldness) where they may also show efficacy. “We expect JAK inhibitors to have widespread utility across many forms of hair loss based on their mechanism of action in both the hair follicle and immune cells,” said Dr. Christiano.
The study is titled, “Oral ruxolitinib induces hair regrowth in moderate to severe alopecia areata.” Additional CUMC authors were Ali Jabbari, Nhan Nguyen, Jane E. Cerise, Charlotte Clark, Grace Ulerio, Megan Furniss, and Roger Vaughan.
*Each individual's treatment and/or results may vary
If you or someone you know has hair loss, hair thinning, baldness, or eyebrow / eyelash concerns, click to start either a long-distance virtual consultation OR an in-person, in-office consultation with Dr. Bauman. You can also Ask Dr. Bauman a Question or simply call Bauman Medical Group at +1-
 FDA Concerns Over Topical Finasteride? Explore Safer, Holistic Hair Loss Treatments
FDA Concerns Over Topical Finasteride? Explore Safer, Holistic Hair Loss Treatments How to relax your way to better hair
How to relax your way to better hair VIDEO: Minimally Invasive FUE Hair Transplant FAQ
VIDEO: Minimally Invasive FUE Hair Transplant FAQ Dr. Alan J. Bauman, M.D.Hair Loss & Hair Transplant ExpertBoca Raton, FL
Dr. Alan J. Bauman, M.D.Hair Loss & Hair Transplant ExpertBoca Raton, FL